An Introduction to Fluid Stewardship - A Belgian perspective
Summary text accompanying the keynote lecture on the 7 D's of fluid therapy during opening ceremony of the 12th International Fluid Academy Day (IFAD) and 9th Benelux Emergency Medicine Symposium (BEMS) held at ULB Erasme auditoria (building W) in Anderlecht/Brussels on Saturday Nov 26th.
Introduction to Fluid Stewardship (IFAD 2022)
On 1 January 2019, the number of approved beds in Belgium was 52,565 of which 34,962 were acute beds, 13,608 were chronic and 3,995 were psychiatric beds. The distribution of the number of beds per province is shown below.
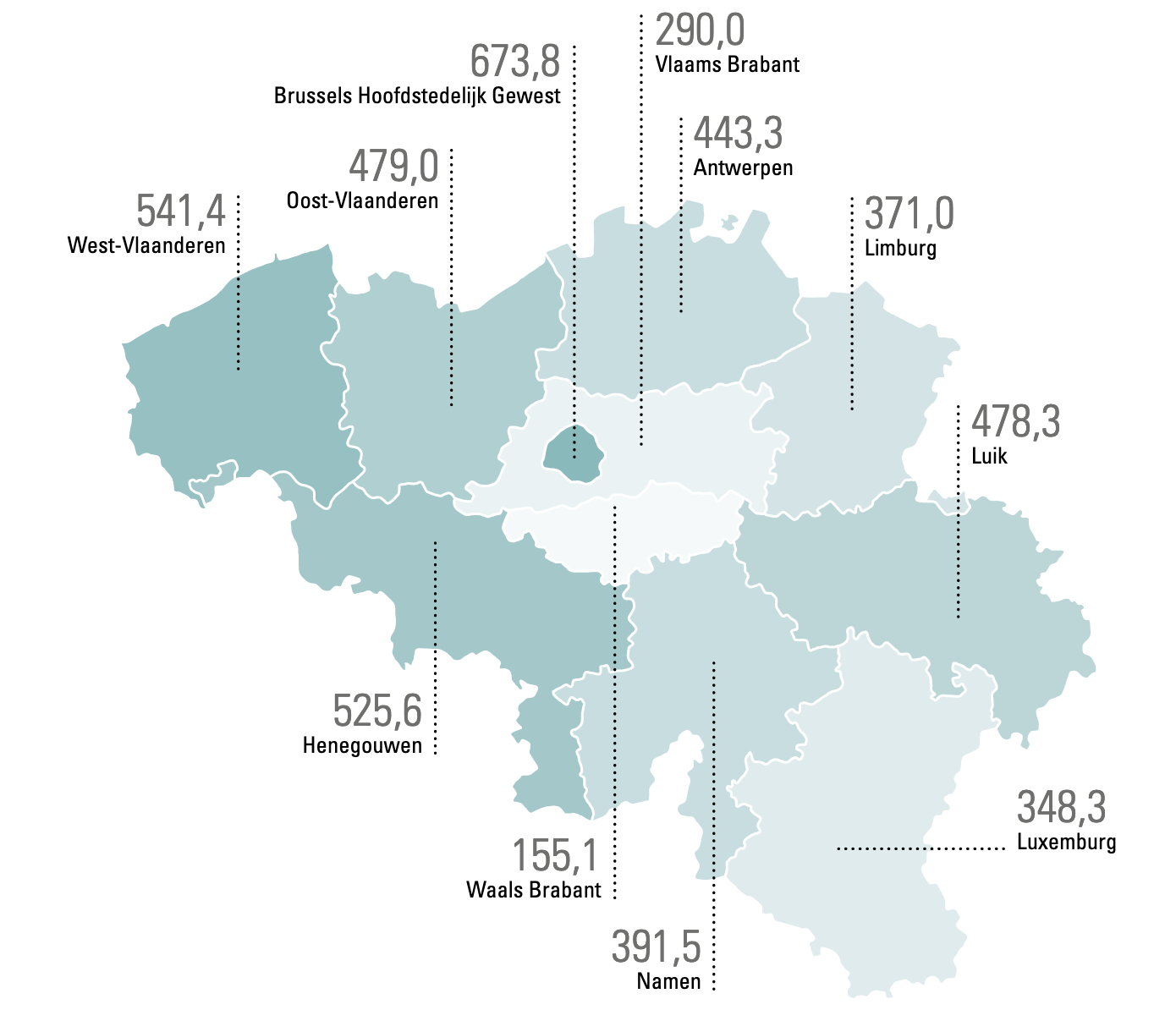
Figure 1. The distribution of the number of approved beds per province (2017)
Analysis of national data on consumption of proprietary medicinal products shows that intravenous (IV) infusion fluids were administered for a total of 14,296,864 litres in 2017. A particularly large proportion of 5,325,440 L of intravenous fluid was given to the patient for administration of other medications (antibiotics, sedation, painkillers, etc..) consisting of 4,262,270 L for medication and 1,063,169 L as dilution solution. This is called fluid creep (1). Maintenance fluids are glucose-containing IV(1) fluids and resuscitation fluids include physiological saline (NaCl 0.9%) or a balanced crystalloid solution (PlasmaLyte®, Hartmann, Ringer acetate) or colloids.
|
Grand Total (L) |
14.296.864 |
|
|
Fluid Creep |
5.325.440 |
37,2% |
|
Maintenance |
3.015.042 |
21,1% |
|
Resuscitation |
5.194.293 |
36,3% |
|
Nutrition |
553.750 |
3,9% |
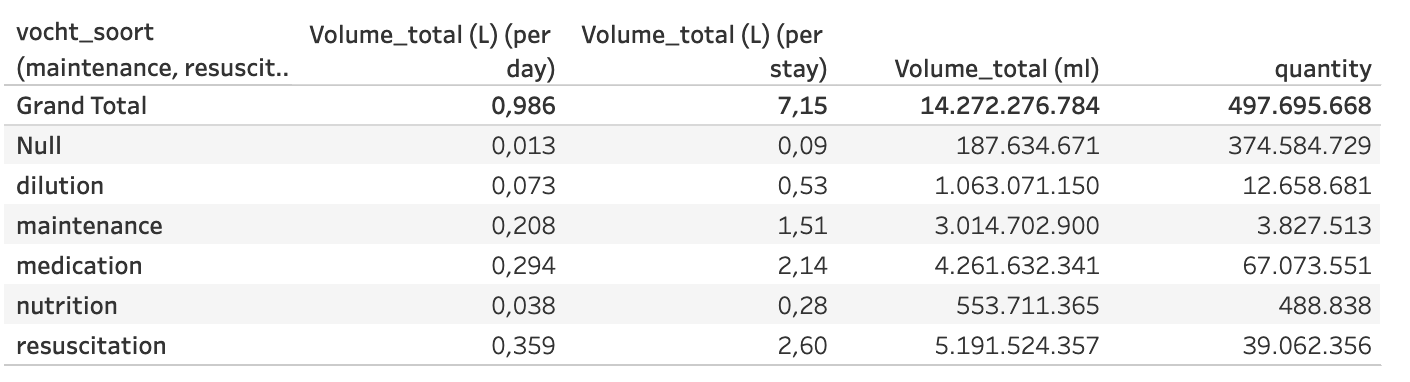
Figure 2 below shows the evolution of the total consumption of IV infusion fluids in Belgium from 2008 to 2017 with a subdivision according to the indication/type of fluid administration (maintenance, resuscitation, medication, nutrition, dilution). In recent years, we have mainly seen an increase in fluid creep. The volume of resuscitation fluids also appears to have increased after the publication of the "large" fluid trials (CHEST and 4S) in the New England Journal of Medicine. These studies showed adverse effects (mainly on kidney function) when using a certain type of colloids, namely hydroxy-ethyl starches. Following the publication of the EMEA PRAC decision, these fluids were banned in the intensive care unit and replaced by crystalloids (NaCl 0.9% and/or balanced/buffered solutions). Since some believe that larger amounts of crystalloids have to be administered to achieve the same effect on hemodynamics and volume expansion, we also see the total consumption increase over the years.
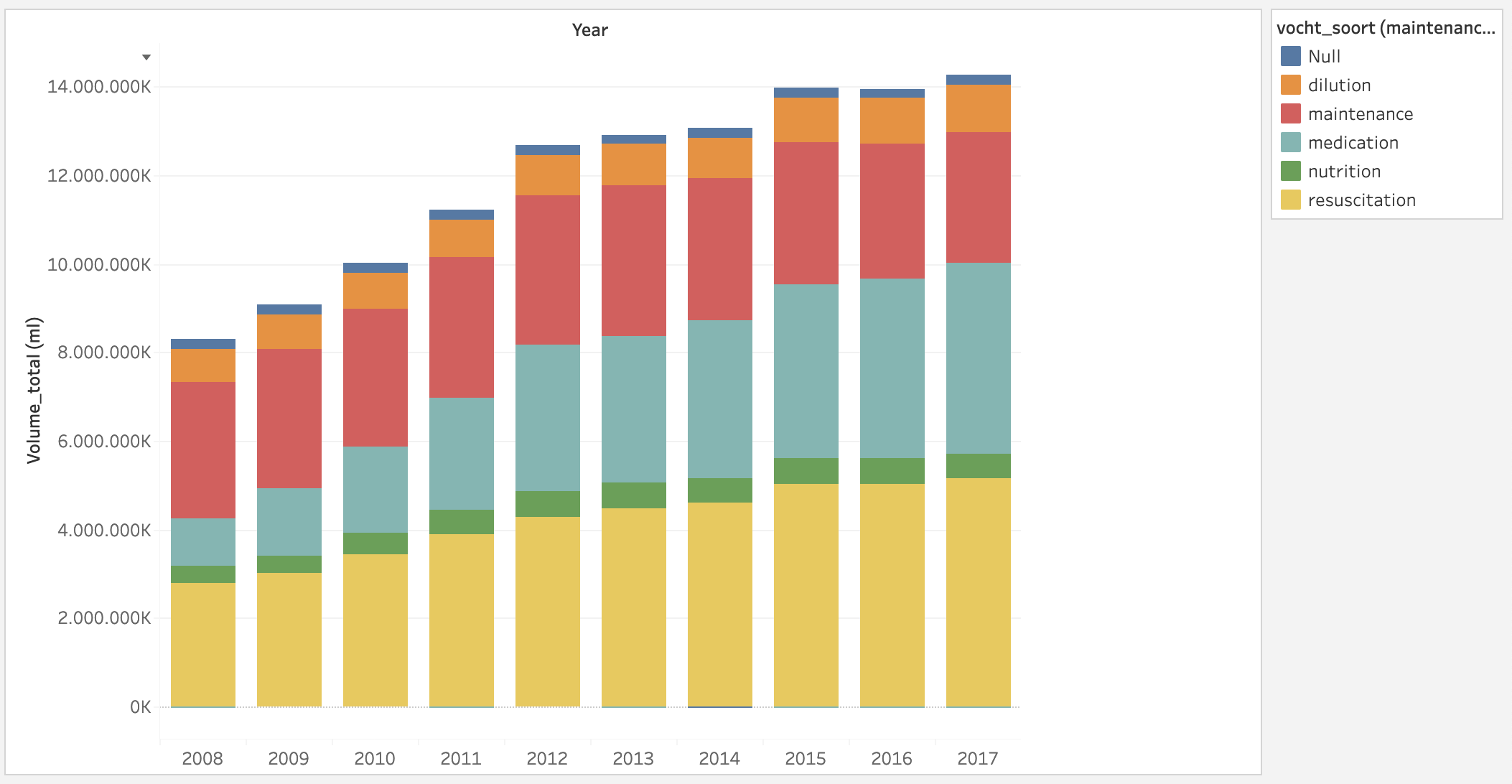
Figure 2. Evolution of total consumption of IV infusion fluids in Belgium from 2008 to 2017 with subdivision by type/indication of fluid
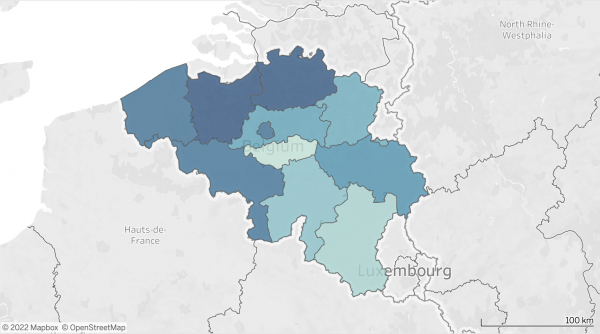
In 2017, there were 1,821,646 classic hospital admissions with a total of 8,379,571.6 acute bed occupying days (average of 4.6 days) and 12,751,522 total bed occupying days (combined average stay acute and chronic of 7 days). The total amount per province is shown on the heat map below (Fig . 3). This more or less corresponds to the number of approved beds (Fig. 1.)
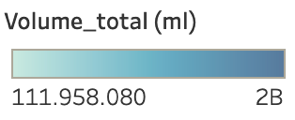
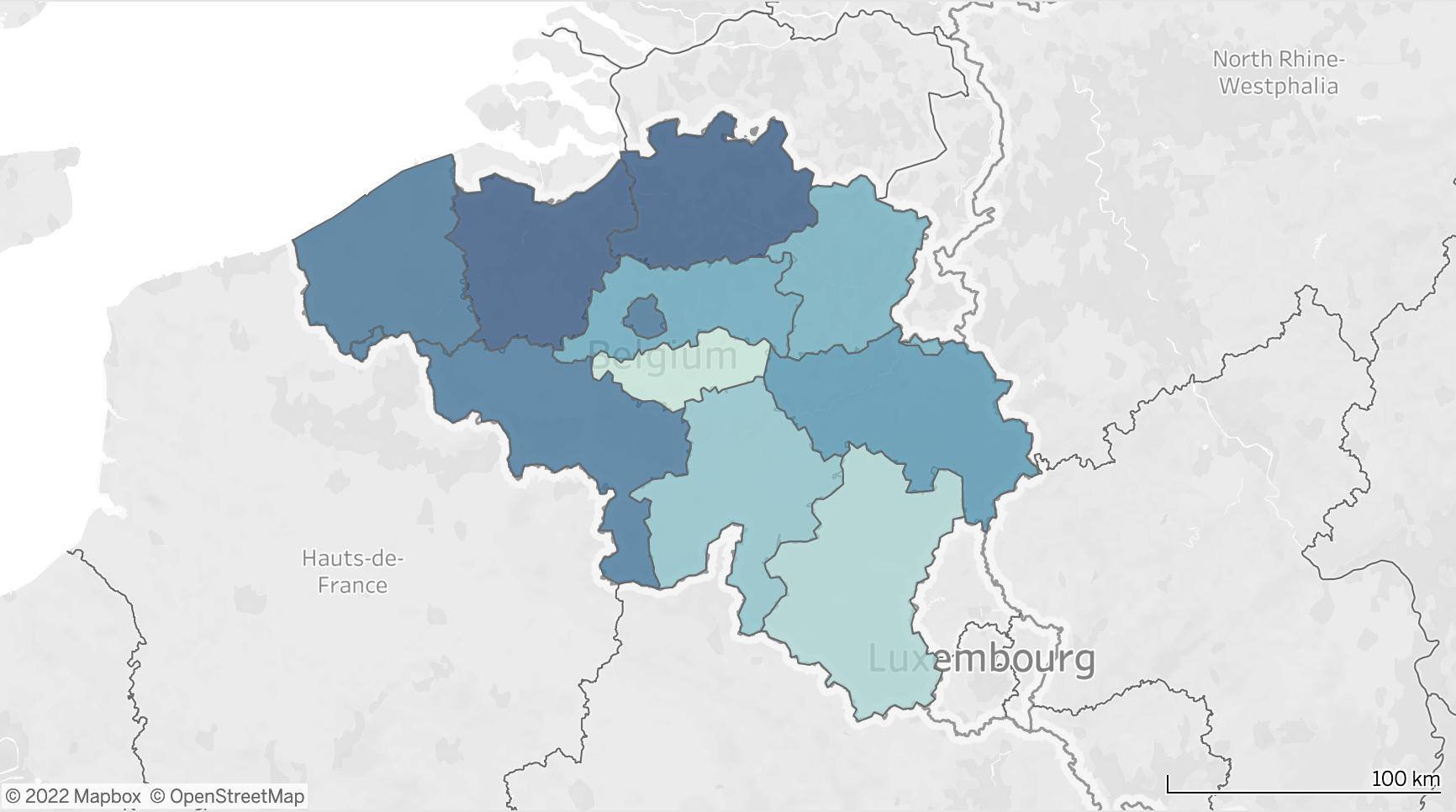
Figure 3. Heat map of total intravenous fluid consumption (in ml) in 2017 per province
Put into perspective, this gives an average of 7.15 liters of IV infusion fluid per stay and 0.99L per bed occupying day. Compared to the international guidelines (NICE, GIFTASUP), this is a very high national consumption (2). (2)The evolution of the total number of L per stay and per day from 2008 to 2017 is shown in Figure 4 (normalized for number of stays and bed occupying days in 2017).
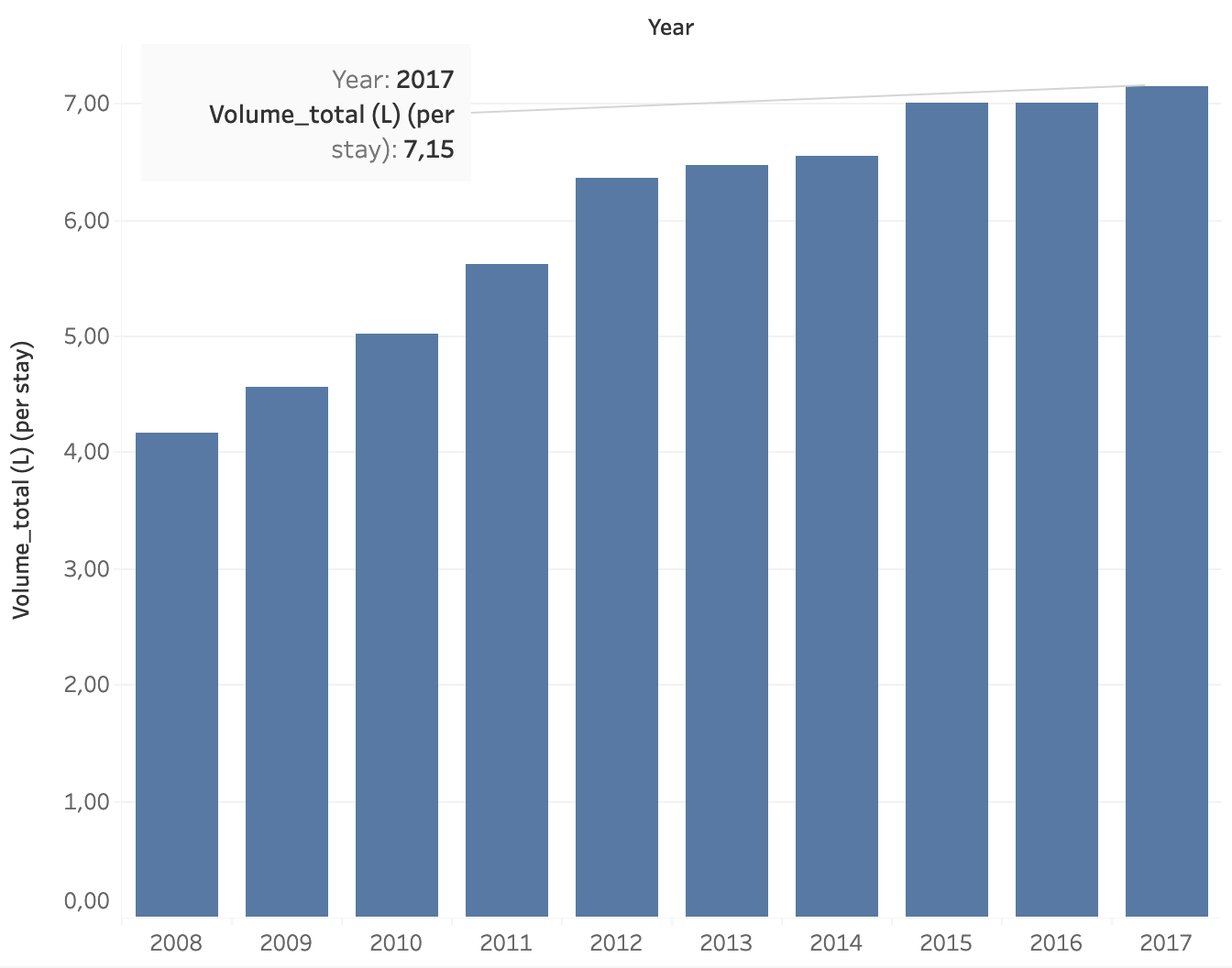
Figure 4. Evolution of the national consumption of infusion fluids (in L) administered per stay (left) and per bed occupying day (right) in Belgium from 2008 to 2017.
Figure 5 shows the evolution of the number of litres of infusion fluids administered as a total without the extra fluids administered as medication or dilution solution. These figures are closer to the literature data with a consumption of 4.4 L per stay and 0.61 L per bed occupying day (see below).
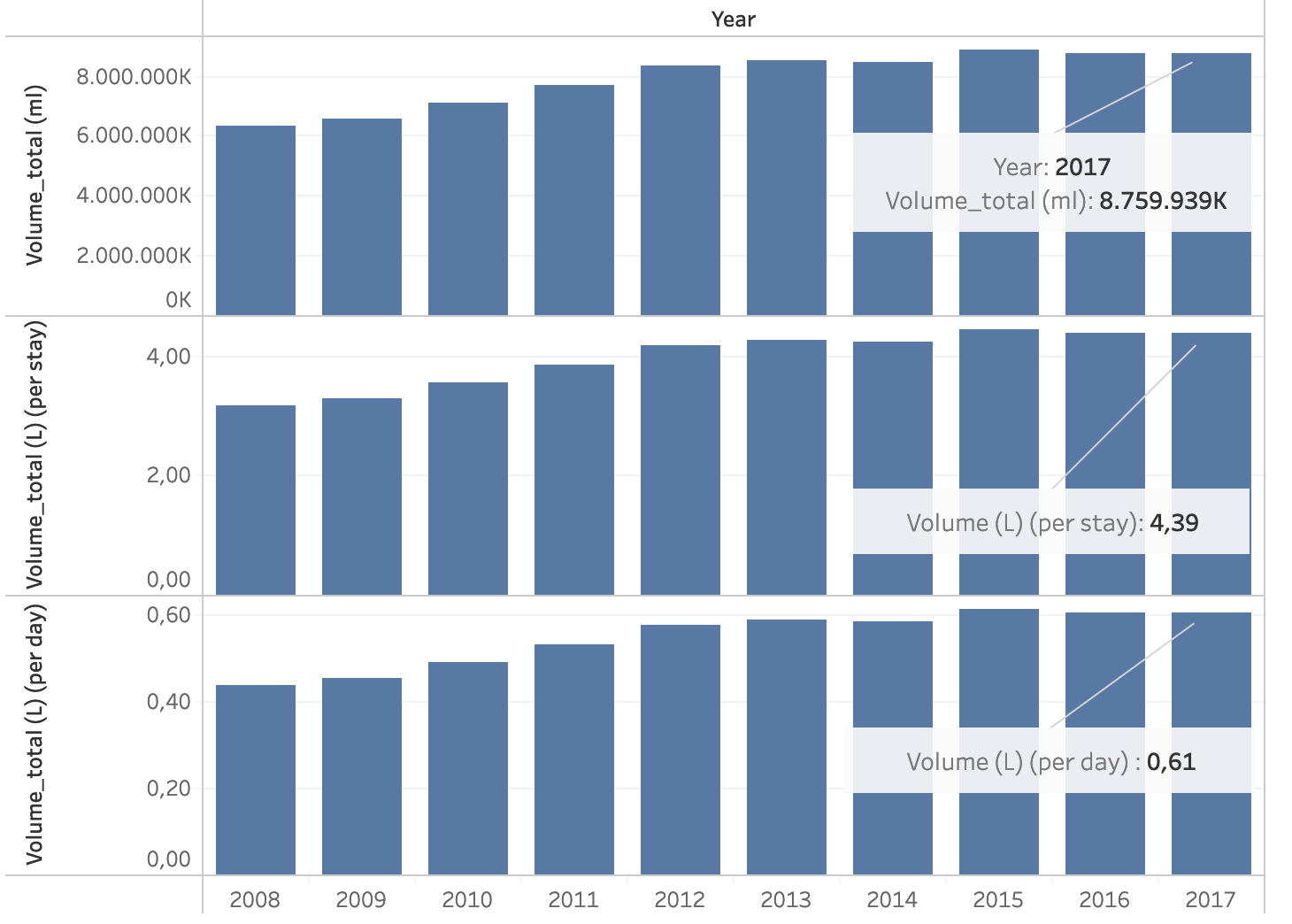
Figure 5. Evolution of the number of litres of infusion flea administered in Belgium as a total (top), per stay (middle) and per lying day (bottom) without medication or dilution solution in the period from 2008 to 2017.
A recent study conducted in Fife in Scotland, by Marcia McDougall and colleagues shows an average consumption of 5 L per stay and 0.65 L per bed occupying day at the start of the fluid stewardship program with a decrease to 3.7 L per stay and 0.4 L per bed occupying day post-implementation (3). Good clinical practice and well thought-out IV fluid use should therefore aim for a consumption of a maximum of 4 L or less per (acute) stay or 0.4 L or less per bed occupying day. With the implementation of a Fluid Stewardship program, it is possible to achieve this objective in any hospital. In Belgium, the analysis of the forfait farmaceutische specialiteiten (FFFS) can be very helpful in carrying out the baseline analysis.
Unfortunately, infusion fluids are all too often do not get the attention they deserve and they are not seen as a real medicine or drugs. As with antibiotic stewardship, we must pay attention to the 4 D's (4)
DRUG
- Approach an IV fluid the same way as any other drug
- Select the type IV fluid with the most suitable composition for the patient
- Think about the indication of why you are using the fluid
- Consider contraindications, comorbidities and side effects
DOSE
- Consider timing, the starting dose, the rate of administration and cumulative dose:
- Fluid tbolus: 4 ml/kg/15 min
- Mini-fluid challenge: 1 ml/kg/5 min
- SSCG: 30 ml/kg/1 hour
- Determine the daily need for
- Water: 1ml/kg/hr of 25 ml/kg/d
- Glucose: 1 – 1.5g/kg/d (to prevent starvation ketosis)
- Sodium: 1 – 1.5 mmol/kg/d
- Potassium: 1 mmol/kg/d
- Chloride: 1 mmol/kg/d
- Consider pharmacodynamics and pharmacokinetics
- Infusion: Same volume effect of crystalloids vs colloids as long as infusion runs
- Distribution: decreased in shock, hypotension, during surgery, after induction and sedation
- Elimination: decreased in shock, hypotension, during surgery, after induction and sedation
DURATION
- Always ask the 4 questions
- When to start with IV liquid?
- When to stop taking IV liquid
- When to start dewatering?
- When to stop dewatering?
- Stop IV infusion if the patient no longer responds to fluid administration without an increase in cardiac output (or blood pressure)
- Monitor for hypo- and hypervolemia
- Use dynamic indices of fluid responsiveness
DE-ESCALATION
- Limit IV fluids as soon as the patient can drink again and take oral fluids
- Give concentrated enteral nutrition
- Start deresuscitation in case of fluid overload and accumulation
- Fluid accumulation causes increased morbidity and mortality
In addition to a high cost price and the fact that fluids consume a significant part of the FFFS (Fig. 6), infusion fluids often cause important morbidity (fluid overload or accumulation with end organ damage, acute kidney failure, electrolyte disorders, etc.) and mortality, especially in the case of their inappropriate use (5).
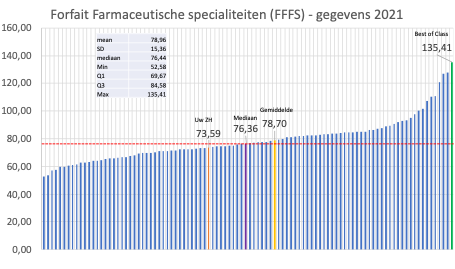
Figure 6. Example of representation of national available data on FFFS with median, mean and best of class.
The goal of fluid stewardship is to obtain a picture of the current infusion practices in some Belgian hospitals and if possible also in Europe (via Ehden project, OMOP-CDM and globally via OHDSI). From this, targeted conclusions can be drawn to prevent overuse and ill-considered infusion use and to develop some useful and clear guidelines to support education and training of doctors and nurses as well as other care givers. Implementation of Fluid Stewardship is the only way to go and this is a team effort and requires change from pharmacists, nurses and doctors.
Definition fluid stewardship
Fluid stewardship is defined as a series of coordinated interventions, introduced to select the optimal fluid, dose and duration of therapy that results in the best clinical outcome, the prevention of side effects and complications and cost reduction (6-8). Recent research suggests that additional knowledge is needed on the proper administration and monitoring of fluids in all hospital departments (3, 9).
Suggested reading
1. Van Regenmortel N, Verbrugghe W, Roelant E, Van den Wyngaert T, Jorens PG. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intensive care medicine. 2018;44(4):409-17.
2. Padhi S, Bullock I, Li L, Stroud M, National Institute for H, Care Excellence Guideline Development G. Intravenous fluid therapy for adults in hospital: summary of NICE guidance. BMJ. 2013;347:f7073.
3. McDougall M, Guthrie B, Doyle A, Timmins A, Bateson M, Ridley E, et al. Introducing NICE guidelines for intravenous fluid therapy into a district general hospital. BMJ Open Qual. 2022;11(1).
4. Malbrain M, Van Regenmortel N, Owczuk R. It is time to consider the four D's of fluid management. Anaesthesiol Intensive Ther. 2015;47:S1-S5.
5. Malbrain M, Langer T, Annane D, Gattinoni L, Elbers P, Hahn RG, et al. Intravenous fluid therapy in the perioperative and critical care setting: Executive summary of the International Fluid Academy (IFA). Ann Intensive Care. 2020;10(1):64.
6. Jacobs R, Jonckheer J, Malbrain M. Fluid overload FADEs away! Time for fluid stewardship. J Crit Care. 2018;48:458-61.
7. Malbrain M, Van Regenmortel N, Saugel B, De Tavernier B, Van Gaal PJ, Joannes-Boyau O, et al. Principles of fluid management and stewardship in septic shock: it is time to consider the four D's and the four phases of fluid therapy. Ann Intensive Care. 2018;8(1):66.
8. Malbrain ML, Mythen M, Rice TW, Wuyts S. It is time for improved fluid stewardship. ICU Management and Practice. 2018;18(3):158-62.
9. Nasa P, Wise R, Elbers PWG, Wong A, Dabrowski W, Regenmortel NV, et al. Intravenous fluid therapy in perioperative and critical care setting-Knowledge test and practice: An international cross-sectional survey. J Crit Care. 2022;71:154122.